While many urological procedures can be safely postponed to limit the exposure of healthcare workers and patients to COVID-19 and conserve medical resources, others – like various cystoscopies – should move forward.
That’s according to recommendations detailed in The Journal of Urology from a collection of urologists from several institutions across the U.S.
They’re not intended to be “strict guidelines,” the authors write, and aren’t endorsed by a medical society or American Urological Association panel. But the framework, gleaned from urologists in different subspecialties, is intended to help triage office-based procedures during the pandemic.
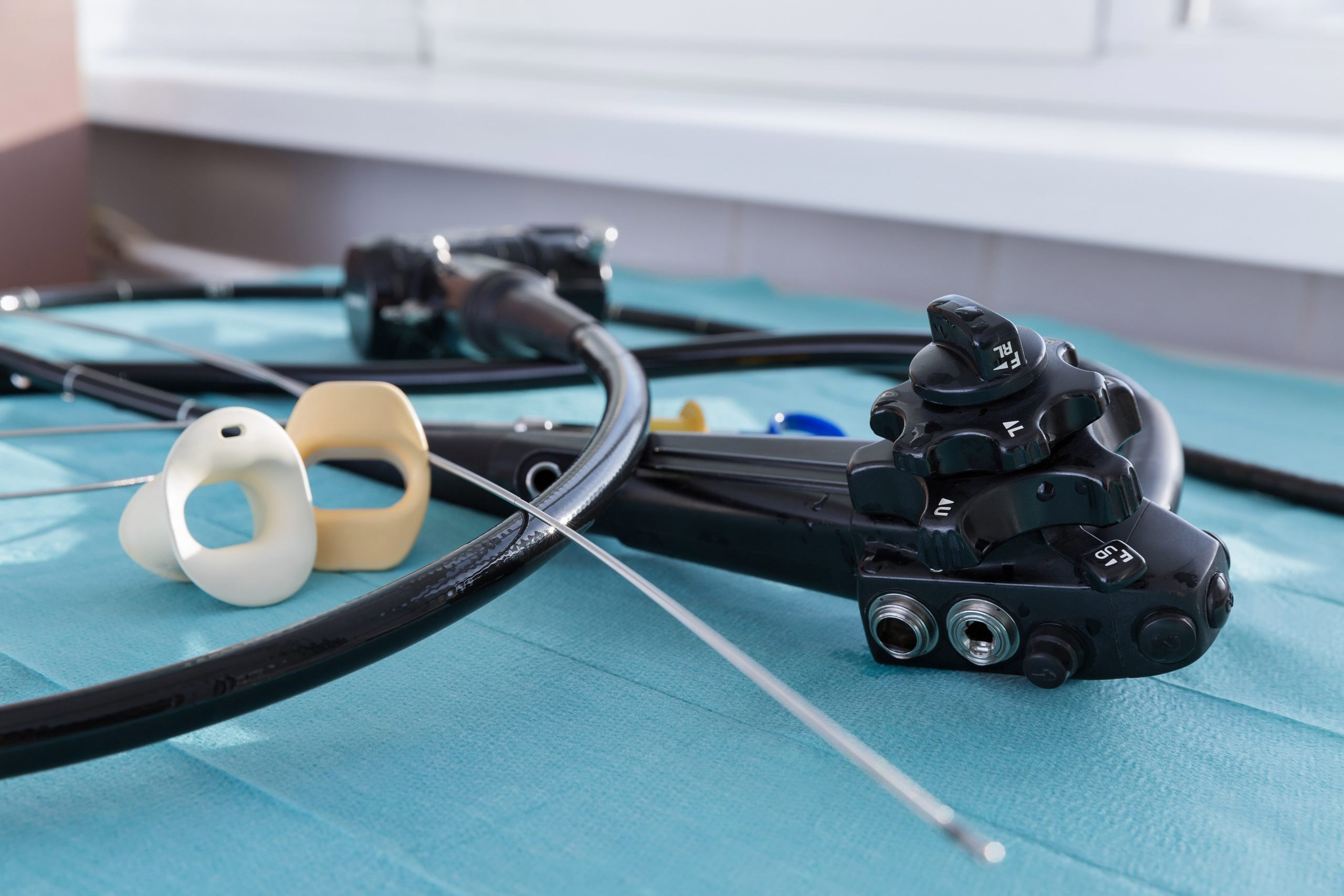
Cystoscopy and ureteral stent removal after ureteroscopy should be performed without delay, according to the recommendations. Diagnostic cystoscopy for gross hematuria, and surveillance cystoscopy for the assessment of response to treatment or surveillance of high-risk non-muscle invasive bladder cancer within six months of initial diagnosis, should also proceed.
Diagnostic cystoscopy for gross hematuria shouldn’t be put off because “diagnostic yield in finding bladder cancer or upper tract malignancy is high in this group.” Regarding surveillance cystoscopy for assessing non-muscle invasive bladder cancer treatment response, there is a high risk of recurrence or progression in the first six months after diagnosis. And cystoscopy and ureteral stent removal after ureteroscopy addresses the risk of encrustation, urinary tract infections, and ongoing symptoms requiring emergency room visit or hospital admission.
Delaying diagnostic cystoscopy for microscopic hematuria with risk factors, including smoking history, for up to three months can be considered unless the patient is symptomatic, according to the authors. In microscopic hematuria without risk factors, diagnostic cystoscopy can be delayed three months or longer.
If it has been at least six months since NMBIC diagnosis, consider delaying surveillance cystoscopy to assess treatment response for as long as three months. In cases of low- to intermediate-risk NMIBC, the procedure could be delayed three to six months.
Triaging procedures is delicate because urological patients are often older and are most at risk of hospitalization or death if diagnosed with COVID-19. Approaches must be tailored to individual settings, with decisions made based on personnel and available resources, “and must always incorporate shared decision making between clinician and patient,” the authors write.
“Every effort should be taken to keep our patients at home, and the rapid expansion of telehealth will allow for many outpatient evaluations to be completed virtually for the foreseeable future,” they add.
Procedures targeted at “the symptomology of conditions,” including stress urinary incontinence, interstitial cystitis, lower urinary tract symptoms, and overactive bladder, can be safely delayed three to six months “depending on individual settings, availability of resources and shared decision making.”



A Learning Center by Ambu USA