Daniel Garrett arrived at his new post as executive director of the American Association for Respiratory Care (AARC) at “a watershed moment” — just as the worst part of the global pandemic was over.
Still, the impact of the pandemic, which has claimed nearly 6.6 million lives, more than 1 million of them in the U.S., is far from over. Not only does SARS-CoV-2 continue to target victims, it’s effects also linger in the form of staff shortages and stress levels of those left to do the work.
A certified association executive, Garrett, who is based in Irving, Texas, was appointed AARC executive director in May 2022. He most recently served as executive director/CEO of the American Society of Transplant Surgeons.
The AARC is a professional association advocating for patients with lung diseases and working on behalf of nearly 40,000 respiratory therapist members who care for them. And each year AARC highlights respiratory therapists during Respiratory Care Week, which this year runs from Oct. 23-29.
As the world tries to right itself after the global pandemic, there is more reason than ever to spotlight the resiliency and optimism of respiratory therapists — and their power to make a difference. One of AARC’s ongoing missions is the high-stakes goal of making sure there is an adequate supply of RTs to serve all the patients who need care.
We spoke with Garrett about this and much more — including details on a new three-year strategic plan that includes workforce recovery and leadership development — in this Q&A, which has been edited for length and clarity.
SUE: What are the biggest challenges facing respiratory therapists today?
Garrett: There’s just a widespread staffing shortage. That burdens all our RTs that are out there working. You throw COVID in there, and you’ve got some burned out people. There’s been a lack of recognition of the hard work done by RTs during COVID. Doctors and nurses got some recognition. But COVID was directly treated by a respiratory therapist, especially if you were in bad shape and on a ventilator. There are still lingering issues and fatigue from the pandemic, and there are people who left because of the pandemic. It’s got to have reverberating effect. They’re burned out.
SUE: What is the AARC doing to address the shortage of respiratory therapists?
Garrett: One of the things that came out in U.S. News & World Report was that respiratory therapy is rated No. 6 in best healthcare jobs. By 2030, 92,000 respiratory therapists will be retired, and employment is only expected to grow 23 percent between 2020 and 2030. I’m afraid it can become more serious if more is not done. AARC is working really hard to fill the pipeline. We’re working together with other agencies, including the National Board for Respiratory Care (NBRC).
SUE: How many additional respiratory therapists are needed?
Garrett: We would need more than 113,000 RTs just to keep status quo. It’s a little scary. This profession is no different from a lot of others that have suffered from the great resignation. I don’t know where the workers have gone.
SUE: What are the key lessons that the pandemic continues to teach?
Garrett: I think really the biggest thing is we’ve got to work in tandem with healthcare institutions and policy makers to share the burden of the gap that exists. Healthcare institutions have got to take notice of this.
SUE: Has the pandemic fundamentally changed the role of RTs?
Garrett: RTs have always been an integral member of the healthcare landscape. I think more people prior to the pandemic didn’t have much recognition of RTs. Now they’re receiving more recognition. Some are traveling to provide care since the pandemic. Some are earning higher salaries.
SUE: What kinds of changes are taking place in the field?
Garrett: Careers are a lot more complex than they were 25 years ago. We need to be on the cutting edge of new treatments. We’re looking at advanced practitioners, advanced practice respiratory therapists (APRTs). They have a higher level of understanding through research and applied research. We’re looking at reevaluating the minimum credentialing from an AA degree to a bachelor’s. Some states call for a BA, and there seems to be a movement in that direction. When there’s a staffing shortage and we’re upping our standards, it’s probably not the best time. But more education translates into better patient care, better patient outcomes.
SUE: What can RTs do in disease management?
Garrett: When RTs operate with a disease management focus, they’re able to use the full extent of their licensing, and the results have been successful. RTs operating in a primary care model have been able to reduce 30-day readmissions. This model means they’ve taught patients how to take care of themselves. It’s not common except in a large pulmonologists’ office. There’s been a lot of talk about putting RTs in a primary care setting to teach the patient how to manage their disease. “Breathing difficulties” would be the diagnosis. An RT can help prevent that from happening.
SUE: How important is the new role of Chronic Obstructive Pulmonary Disease (COPD) navigator?
Garrett: COPD is the third-costliest disease in the U.S. COPD navigators who follow patients into post-acute care reduced readmissions by 50 percent. The role of COPD navigator is incredibly important to patients. The navigator really bridges that continuum of care for the patient within the hospital and from acute care to post-acute care.
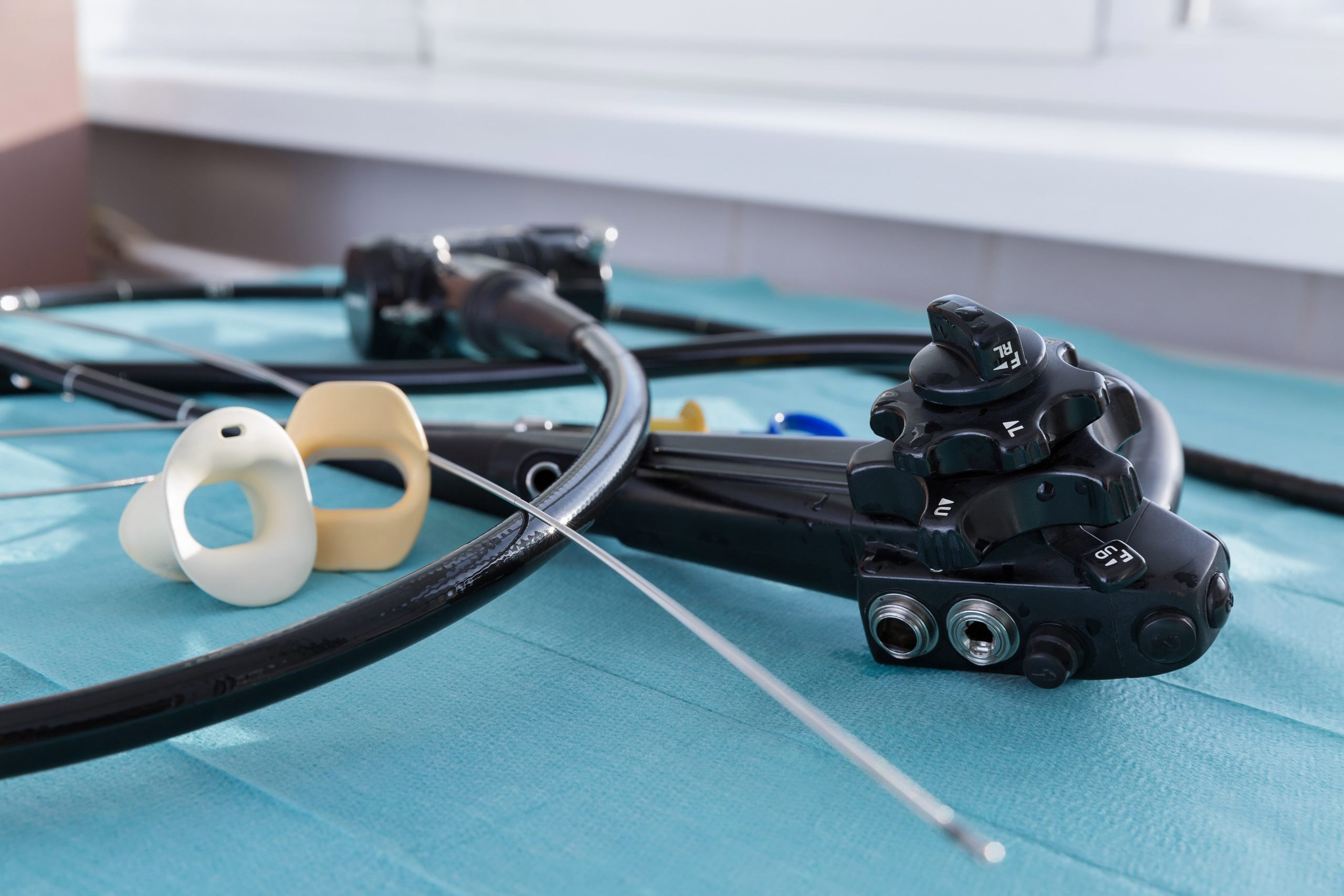
SUE: What do you view as the role of single-use devices?
Garrett: In the past few years, we've seen a push toward using single-use medical devices in an effort to improve infection control. Bronchoscopes, used for examining and treating the airways, were traditionally reusable devices that required careful cleaning and sterilization between uses. However, single-use bronchoscopes became increasingly popular with the outbreak of COVID-19 and the heightened focus on preventing cross-contamination and transmission of the virus. These disposable scopes eliminate any concerns about possible contamination from reprocessing and provide peace of mind for both health care workers and patients. It is likely that this trend toward single-use medical devices will continue in the future as a proactive measure to prevent infections and ensure patient safety.
SUE: What else would you like to share?
Garrett: AARC just completed a three-year strategic plan that includes workforce recovery and leadership development within our own ranks. We will do everything we can to promote diversity, equity and inclusion, from our words to our actions. We are also enhancing and revamping our website, reimagining the AARC brand as an organization.



A Learning Center by Ambu USA